

Dr Karen Fong is a practising small animal veterinarian based in the Midlands, UK. She graduated from the University of Edinburgh with distinction in 2021 and has also passed The North American Veterinary Licensing Examination (NAVLE) . During her time in practice, she has developed a strong interest in medicine and ophthalmology. She also enjoys creating study material for vet students. In her free time, Dr. Fong’s artistic talents shine through her oil paintings, reflecting her multifaceted interests and creative spirit. She is also a proud cat mum!
Background
Feline Hyperthyroidism is the most common endocrine disease in cats, and a topic that professors like to put in exams! The condition is caused by primary functional thyroid adenomas or hyperplasia, which produces excessive circulating thyroid hormone. Middle-aged to old, non-pedigree cats are predisposed. There are various risk factors postulated, such as exposure to canned cat food, insecticides etc.
Presentation
Affected cats are often brought in due to a wide range of signs as thyroid hormone is involved in the sympathetic nervous system and many other body systems.
History from owners
- Weight loss and/or muscle wastage despite polyphagia
- Due to increased metabolism and body temperature
- Polydipsia and polyuria (PUPD)
- Due to thyroid hormone antagonism against aldosterone, electrolyte disturbances, psychogenic polydipsia, or concurrent renal dysfunction.
- Vomiting and diarrhoea
- Due to intestinal overload and hypermotility. In some cases, low cobalamin levels (VitB12) may also be a factor.
- Behavioural changes, such as restlessness and vocalisation, or excessive grooming
- Due to increased sympathetic drive
On clinical exam
- Low body condition and/or muscle atrophy
- Tachycardia
- Due to increased sympathetic tone
- Systolic murmurs, gallop rhythm
- Due to dynamic ventricular outflow obstruction and rapid ventricular filling.
- Congestive heart failure (CHF)
- Hyperthyroidism predisposes to hypertrophic cardiomyopathy (HCM)
- Hypertension
- Tachypnoea
- Palpable goitre
- Goitre can be palpated with the cat’s neck extended, and thumb and forefinger at either side of the trachea.
- Cervical ventroflexion (“swan neck”)
- Severe muscle weakness, hypokalaemia
- Matted coat
(Halfacree, n.d.)

Differentials
💡 Hyperthyroid cats often present with vague signs and frequently have concurrent conditions, particularly CKD! Therefore, differentials should be carefully considered and ruled out.
- Diabetes mellitus (DM)
- Chronic Kidney disease (CKD)
- Chronic enteropathy (CE)/ Inflammatory bowel disease (IBD)
- Exocrine pancreatic insufficiency (EPI)
- Primary HCM and CHF
- Neoplasia
Diagnosis
Haematology
- Erythrocytosis
- Stress leukogram
- SMILED (Segmented neutrophils, Monocytes Increased; Lymphocytes, Eosinophils Decreased)
biochemistry
- Elevation in hepatic enzymes (ALT, ALKP)
- Azotaemia
- Commonly due to concurrent CKD. However, this can be masked by an increased glomerular filtration rate (GFR) due to PUPD
- Hyperglycaemia
- Stress hyperglycaemia
- Hyperphosphataemia
- Altered bone metabolism (and concurrent CKD)
Urinalysis
- Decreased USG
- Evidence of bacterial UTI
- Common complication due to diluted urine
- Proteinuria
- Due to hypertension or concurrent renal disease
Thyroid hormone assay
- Total T4 (TT4)
- Diagnostic if elevated TT4
💡 Results of TT4 can sometimes be ambiguous or falsely suppressed due to diurnal fluctuations or Euthyroid Sick Syndrome (TT4 levels suppressed by non-thyroidal illness). In such cases, retesting or freeT4 assay is recommended.
- Free T4
- Tested by equilibrium dialysis
- less influenced by Euthyroid sick syndrome
- Other less common tests
- TSH stimulation test
- Free T3 levels
Scintigraphy
- Radioactive iodine isotope is used to assess the activity of thyroid tissue. Increased uptake of iodine by hyperactive thyroid tissue allows detection of ectopic tissue and metastasis.
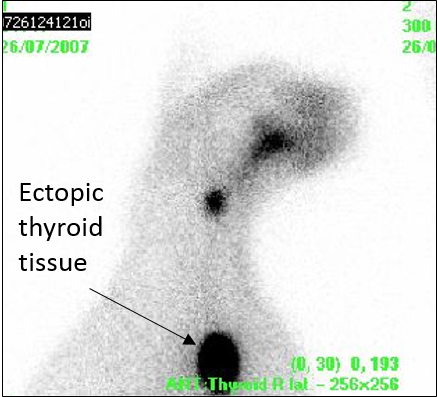
(Halfacree, n.d.)
💡 Concurrent CKD is often masked by uncontrolled hyperthyroidism, making diagnosis difficult. Creatinine may appear normal due to increased GFR and muscle atrophy. Elevation in urea may be mistaken for proteolysis in cats with poor body conditions. In such cases, the most reliable test is SDMA (symmetric dimethylarginine), which is not affected by muscle mass. It is highly important to be aware that treatment of hyperthyroidism can uncover azotaemia, leading to a poorer prognosis if not managed appropriately. In addition, over-treatment (hypothyroid state) can reduce mean survival time (MST)!
Treatment
Initial stabilisation
💡 A period of stabilisation to achieve a euthyroid state is recommended to allow evaluation of renal function before committing to irreversible treatment methods (surgery or radioiodine).
- Medical treatment
- Oral methimazole or carbimazole for 2-4 weeks, then screen for azotaemia
- Iodine-restrictive diet
- Less commonly used
- Restricting dietary iodine levels leads to a decrease in the synthesis of thyroid hormones. The diet should be fed exclusively for 2-4 weeks, then evidence of CKD evaluated.
Long-term management
There are different methods of managing hyperthyroidism, and each comes with its pros and cons. (The professors love asking you to evaluate them!)
- Radioactive Iodine
- Gold standard
- Radio-iodine 131 is injected subcutaneously and is concentrated by the abnormal thyroid gland, destroying the neoplastic cells, including ectopic tissue. There is a high success rate of 95%, however, cats have to be isolated with minimal handling for 3 weeks.
- 👍
- Curative
- Able to target ectopic tissue and carcinomas
- No anaesthetic or surgical risks
- 👎
- Irreversible and risk of over-treatment
- Not suitable for CKD patients
- Careful patient selection is required. It is not suitable for patients with concurrent diseases that require daily medication (such as DM)
- expansive and not readily available
- Irreversible and risk of over-treatment
- Long term medication
- oral methimazole (BID orally) or carbimazole (SID orally)
- The medication inhibits thyroid peroxidase, limiting iodine uptake and thyroid hormone synthesis
- 👍
- Reversible, no risk of over-treatment
- medication can be titrated to appropriate GFR levels and is more suitable for cats with concurrent CKD
- No anaesthetic or surgical risk
- Readily available
- able to spread out costs
- Reversible, no risk of over-treatment
- 👎
- Not curative
- Side effects
- transient vomiting, diarrhoea, anorexia
- serious complications such as hepatopathy, facial excoriation or blood dyscrasias
- switching drugs is not always useful, as they have the same active ingredient
- efficacy depends on client and patient compliance
- total costs can add up over the years
- Surgery (Thyroidectomy)
- Thyroid glands at either side of the trachea (2nd – 5th tracheal rings) are resected while preserving the 4 parathyroid glands and surrounding structures such as the laryngeal nerves and carotid arteries.
- 👍
- Curative
- readily available
- Relatively non-expansive compared to other treatments
- No drug dosing needed
- 👎
- Anaesthetic and surgical risks
- Surgical complications
- Laryngeal paralysis
- Hypoparathyroidism leading to hypocalcaemia
- irreversible and risk of over-treatment
- risk of recurrence, if unilateral thyroidectomy is done or there is ectopic tissue.
- Iodine-restrictive diet
- Not commonly used as long-term management
- 👍
- No anaesthetic or surgical risks
- No drug dosing needed
- Reversible
- Readily available
- Able to spread out costs
- 👎
- Not curative
- Difficult to implement
- The diet has to be fed exclusively and is not very palatable. It is not suitable for outdoor cats, or in multi-cat households. It is also not suitable for cats with concurrent diseases that require dietary management
- Total costs can add up over the years
Prognosis
The prognosis is good with radioiodine therapy or thyroidectomy, and moderate with medical management. However, concurrent conditions such as CKD or CHF must be monitored and treated.
References and Resources
- Vetlexicon.com. 2022. Hyperthyroidism in cats | Vetlexicon Felis from Vetlexicon | Definitive Veterinary Intelligence. [online] Available at: <https://www.vetlexicon.com/treat/felis/diseases/hyperthyroidism> [Accessed 29 August 2022].
- Torrance, A. and Mooney, C., 1998. BSAVA manual of small animal endocrinology. Shurdington, Cheltenham, U.K.: British Small Animal Veterinary Association, pp.92 – 110.
- https://icatcare.org/advice/hyperthyroidism/
- Halfacree, Z., n.d. Thyroid gland: ectopic thyroid tissue – scintigram. [image] Available at: <https://www.vetlexicon.com/treat/felis/illustration/thyroid-gland-ectopic-thyroid-tissue-scintigram> [Accessed 6 September 2022].
- Herritage, M., n.d. Hyperthyroidism. [image] Available at: <https://www.vetlexicon.com/treat/felis/illustration/hyperthyroidism> [Accessed 6 September 2022].